There is a move afoot to incorporate Intermittent Hypoxic Training (IHT) in a number of different medical fields. Sports performance and general well-being may be one of the most important of these fields. Intermittent Hypoxia has been the subject of considerable research in recent years. It can trigger a bewildering array of both detrimental and beneficial effects in multiple physiological systems. When administered properly it can have many beneficial aspects. If one utilizes the proper equipment, this will eliminate the detrimental aspects. One method of Intermittent Hypoxic Training (IHT) is training at a high altitude. This is the oldest and most common IHT.

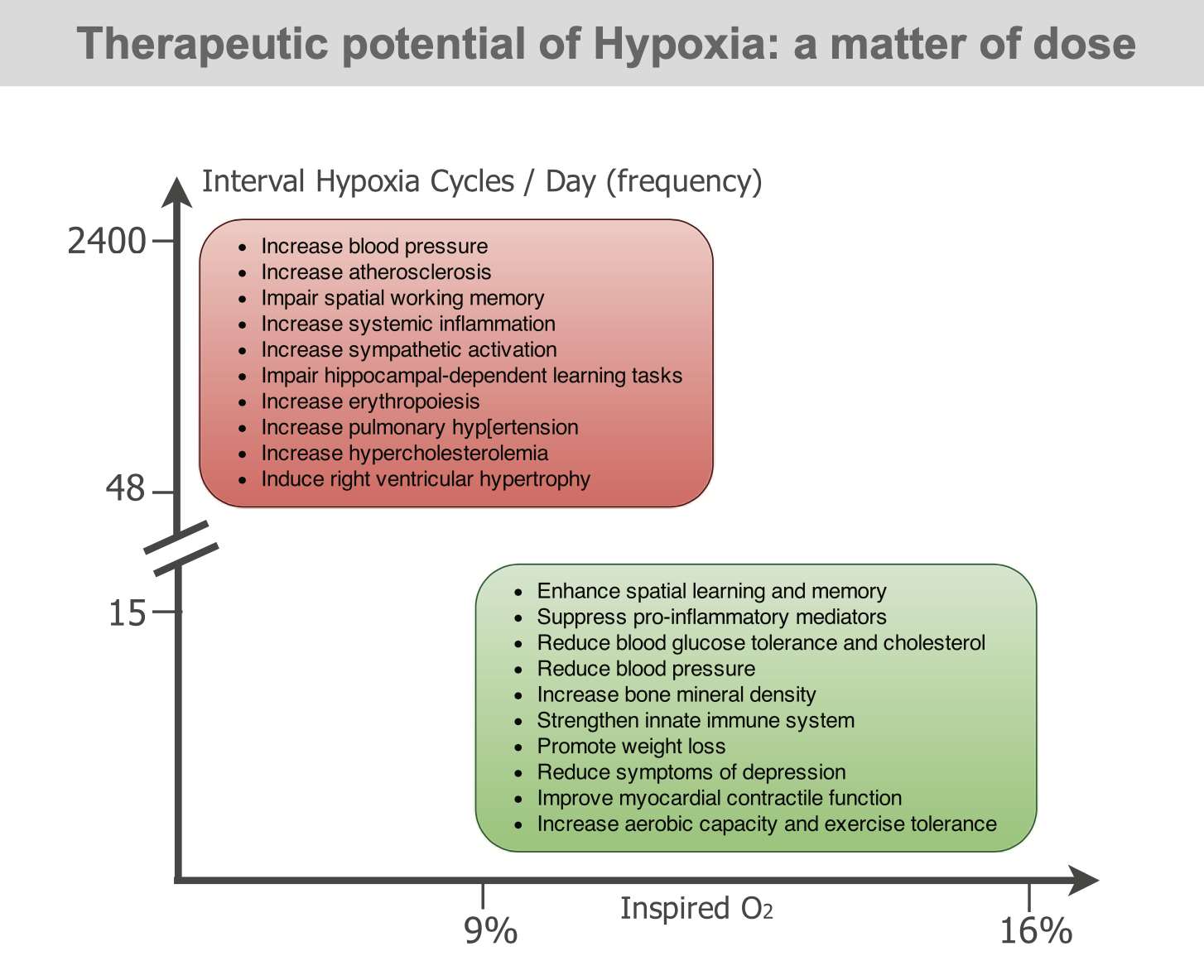
For years, many professional and Olympic athletes have used altitude training for a competitive edge. Training under hypoxic conditions, particularly IHT during a training session, improves hematological and muscle adaptations and this has been used to improve the exercise performance of athletes by sports medicine community. IHT is simply a modified version of the “live high train low philosophy”, where an individual spends most of their time residing at high altitude prior to descending during training session. Modest hypoxia (9–16% inspired O2) and low cycle numbers (3–15 episodes per day) most often lead to beneficial effects without pathology, whereas severe hypoxia (2–8% inspired O2) and more episodes per day (48–2,400 episodes/day) elicit progressively greater pathology. Accumulating evidence suggests that “low dose” intermittent hypoxia (modest hypoxia, few episodes) may be a simple, safe, and effective treatment with considerable therapeutic potential for multiple clinical disorders. Even if one were to train at a high altitude there are still methods to make the training much more efficient. The intermittent hypoxia aspect adds to this efficiency.
WHAT IS THE SCIENCE INVOLVED WITH INTERMITTENT HYPOXIC TRAINING?
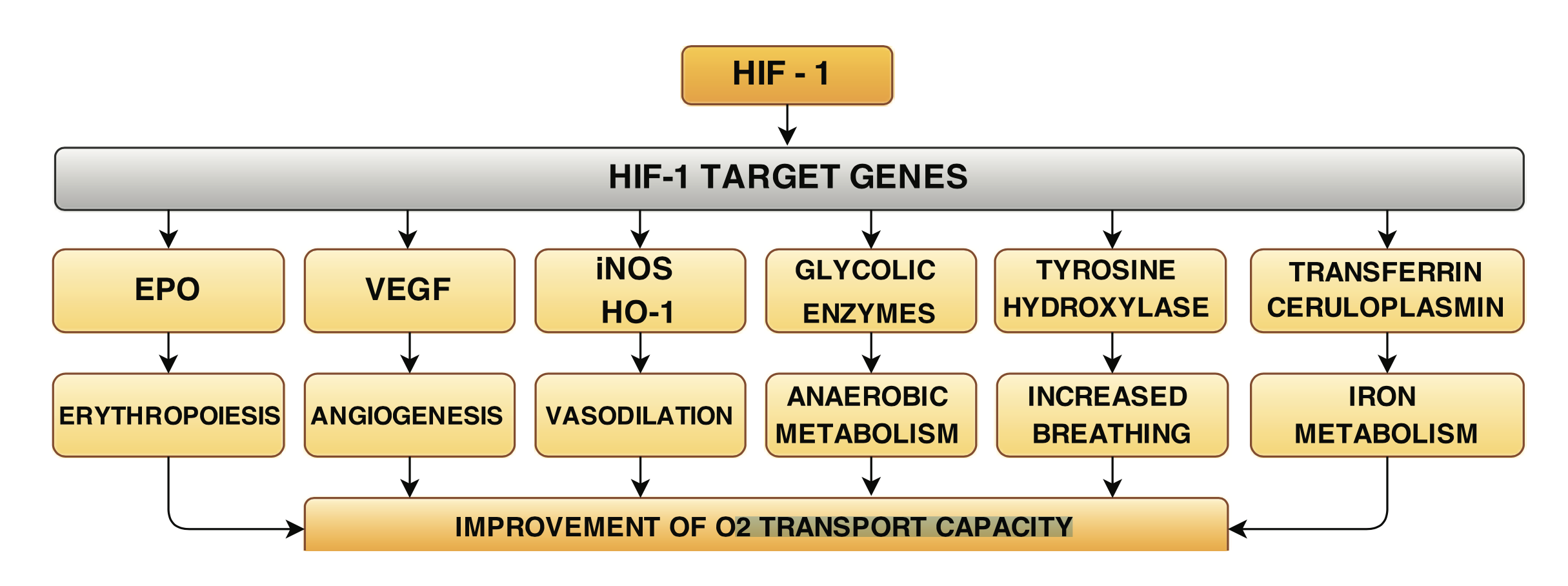
The above diagram shows some of the science associated with Intermittent Hypoxic Training (IHT). One of the main aspects of Intermittent Hypoxic training is the stimulation of HIF-1, also known as Hypoxia Inducible Factor-1. HIF-1 is an extremely important growth factor. HIFs are transcription factors (factors that directly affect various genes) that respond to decreases in available oxygen (hypoxia) in the cellular environment. Hypoxia-inducible factors (HIFs) are key molecules that regulate cellular responses to inflammation and hypoxia. These responses are essential for the normal cell function and survival. In hypoxic conditions, HIF-1 serves as a transcription factor that regulates over 100 genes essential for survival in oxygen-deprived conditions. The next diagram shows how cell biology comes into play with hypoxia compared to Normoxia (normal oxygen concentration and pressure found at sea level at sea-level).
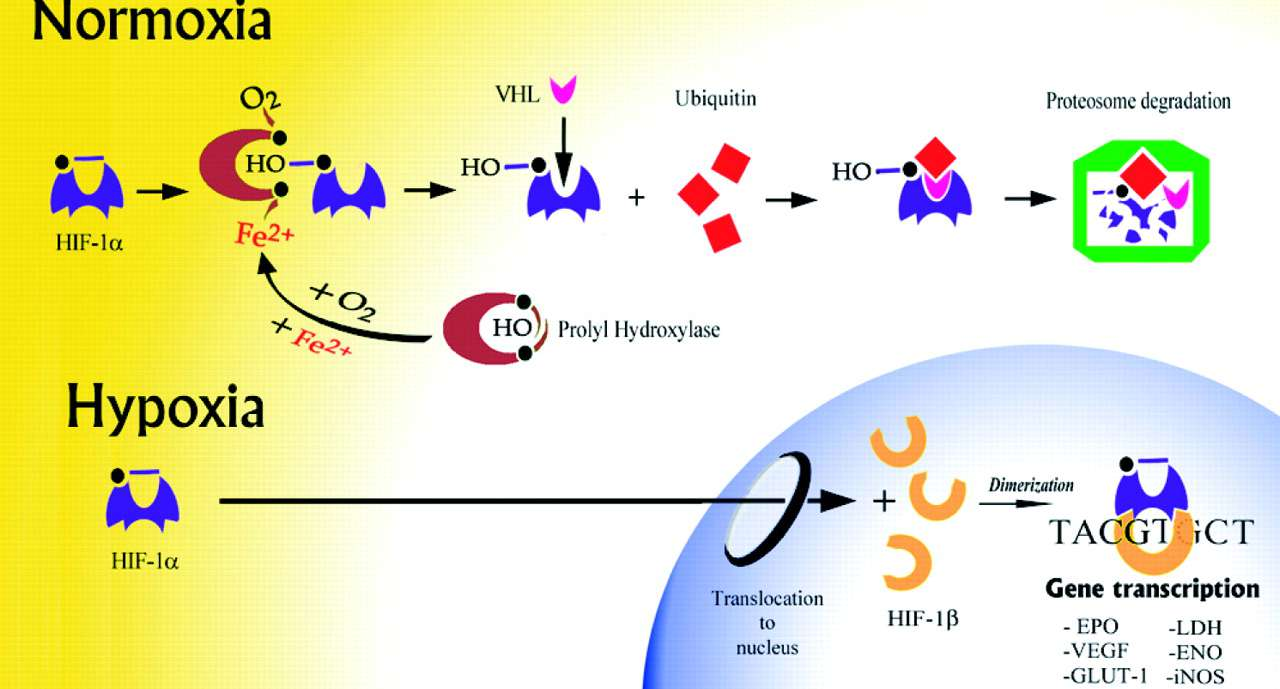
What can be seen here is that at sea-level HIF-1 is disabled while with hypoxia there is stimulation of HIF-1 resulting in entering the nucleus of the cell. Once in the nucleus it stimulates genes which are responsible for the production of a number of compounds responsible for many of the beneficial effects of hypoxia. There are three forms of HIF, HIF-1 and HIF-2 and HIF-3. HIFs are important for the well-being of a variety of different types of tissues. HIF-1 also has an important role in the regeneration and maintenance of essential organ functions that are highly oxygen-dependent such as the brain and the heart. HIFs are important in the production of a compound called Erythropoietin (EPO) which results in the production of various blood cells especially red blood cells. Additionally, it will also release numerous stem cells into the circulation. HIF is of prime importance in the production of a growth factor called SDF-1 (also called CXCL 12). In humans, SDF-1 has been implicated in a wide variety of biomedical conditions involving several organ systems. It essentially allows stem cells to be attracted to areas where they are needed. In adulthood, CXCL12 plays an important role in angiogenesis (blood vessel formation) by recruiting endothelial progenitor cells (EPCs) from the bone marrow. Ultimately, the all of these effects contribute to improved oxygen transport capacity.
HIF-1 controls oxygen delivery, by regulating angiogenesis and vascular remodeling. It also controls oxygen utilization, by regulating glucose metabolism and redox homeostasis (keeping free radicals in balance). HIF-1 activity is induced by hypoxia through changes in HIF-1 mRNA (messenger RNA) protein levels in brain, heart, kidney, lung and skeletal muscle. mRNA regulates expression of a large number of genes whose protein products play critical roles in mediating vascular responses to hypoxia and ischemia. The mRNA gives the genes messages to produce certain proteins. These proteins in turn have many beneficial effects on the body.
There are a number of other influences hypoxic conditions have on our health. The following illustration demonstrates some of these conditions. We will look at these individually.
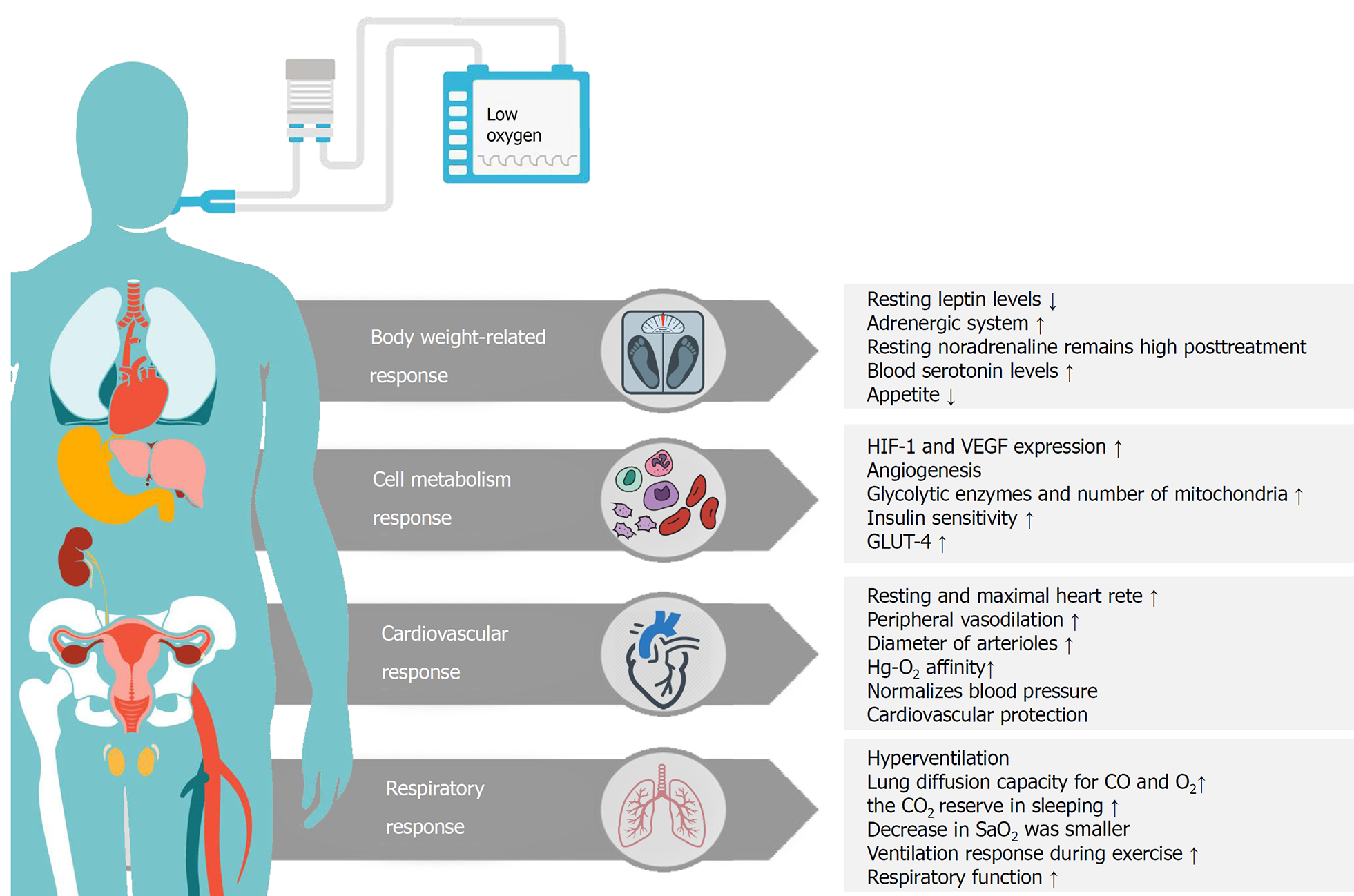
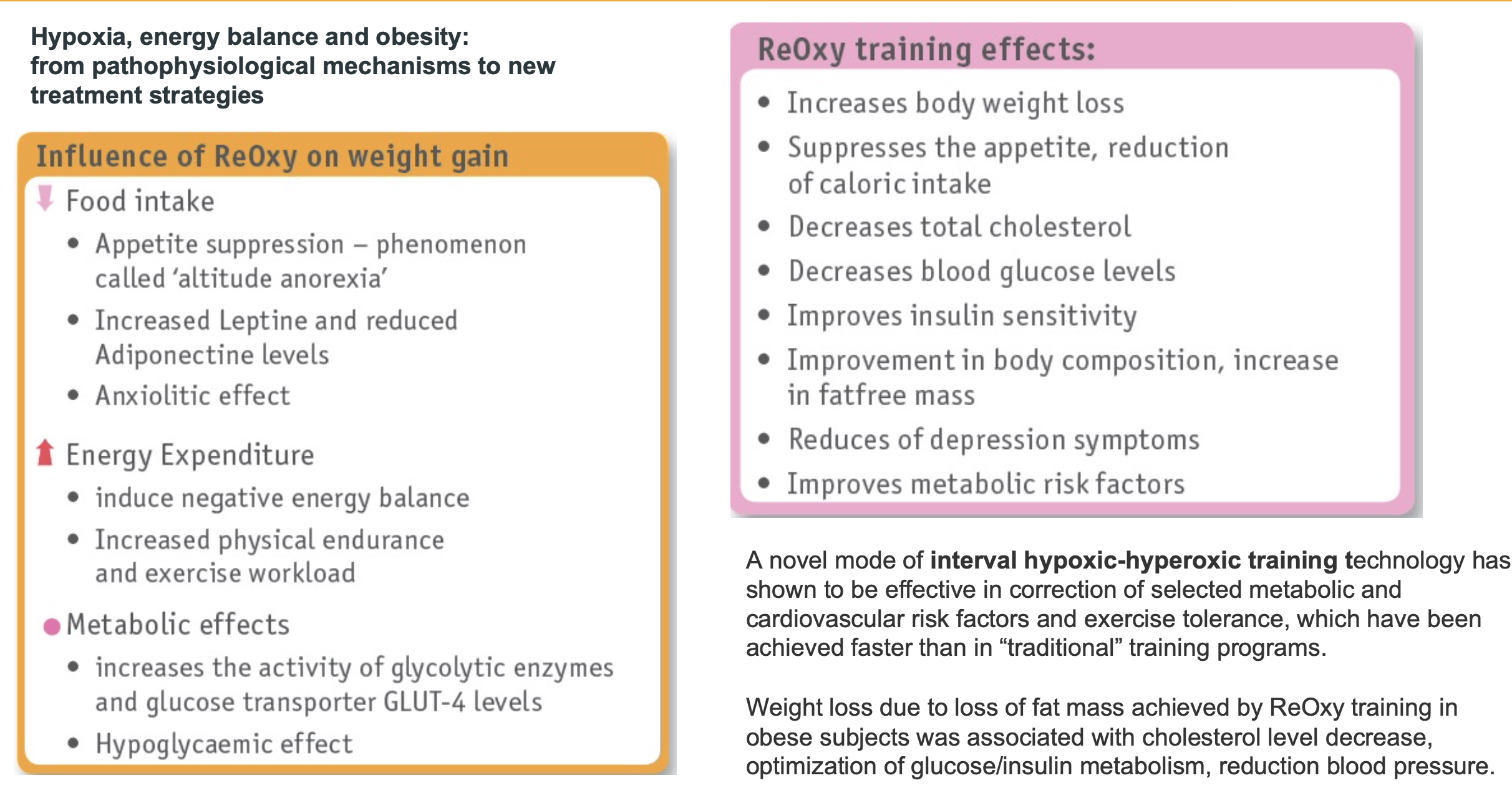
One of the above responses is how intermittent hypoxia can affect body weight. As can be seen, the reduction in body weight is accomplished by a number of different mechanisms. One of these mechanisms is the reduction of appetite. Another one is the reduction of Leptin levels. Leptin is a hypoxia-inducible hormone released from fat cells in adipose tissue. Leptin acts upon the brain, in particular to an area called the hypothalamus. Leptin does not affect food intake from meal to meal but, instead, acts to alter food intake and control energy expenditure over the long term. Leptin has a more profound effect when we lose weight and levels of the hormone fall. This stimulates a huge appetite and increased food intake. The hormone helps us to maintain our normal weight and unfortunately for dieters, makes it hard to lose those extra pounds! HIT increases Leptin. In the next illustration we see some of the methods hypoxia training affects weight loss. The studies have shown that the weight loss benefits are multifaceted and include aspects that have already been mentioned such as decreased Leptin levels which can then suppress appetite.
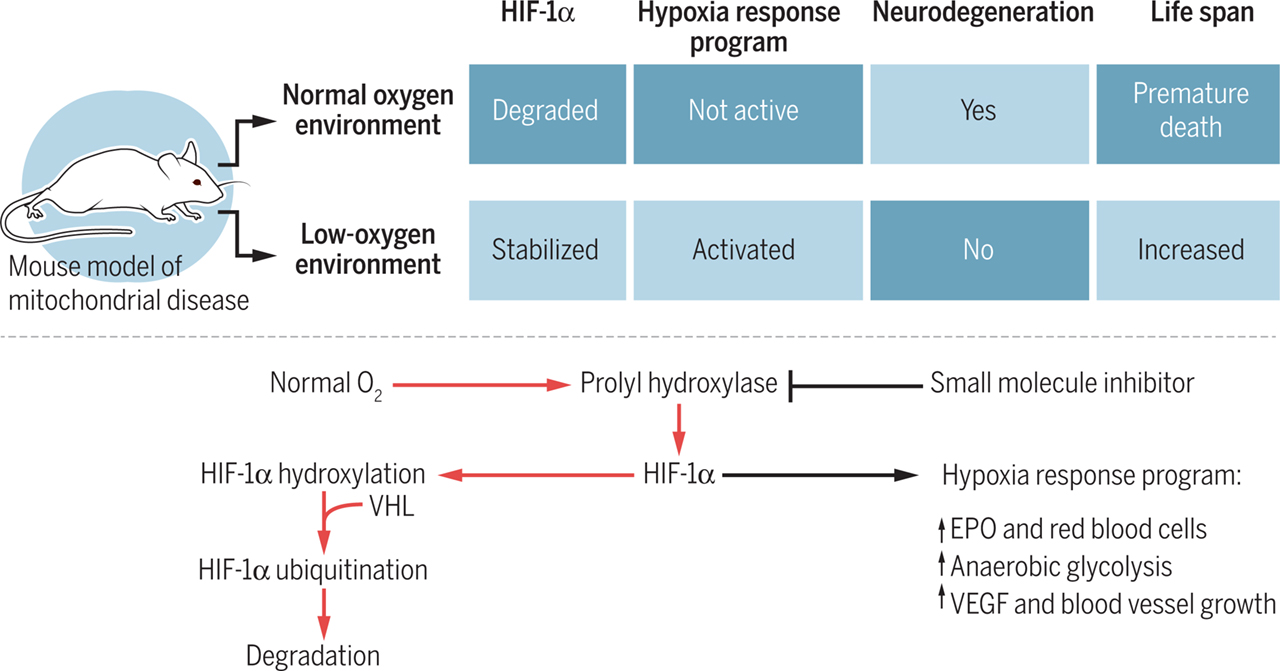
Another response mentioned above is cell metabolism. The cell metabolism is affected on a number of different levels. One such effect includes an increase sensitivity to insulin by the body. Typically, when one has diabetes the insulin sensitivity is much lower and thus more insulin is needed to do the job. In addition to promoting O2 delivery, HIF-1 also activates the transcription of genes encoding enzymes, transporters, and mitochondrial proteins that decrease O2 utilization. Thus, HIF functions as a master regulator to switch cells from oxidative metabolism to glycolytic metabolism. One condition in the body which can be favorably affected by hypoxia training is the health of our mitochondria. This is probably the most piece of all. As science is now discovering, the health of our mitochondria typically will determine out health. Many diseases have their roots in mitochondrial dysfunction. Many studies suggest that hypoxic gas mixtures may be useful in treating or preventing mitochondrial disorders. This approach is seemingly counterintuitive, since oxygen is a key substrate for the respiratory chain which produces the body’s energy currency ATP. However, hypoxia activates an adaptive program that allows us to cope with limiting oxygen levels. This program decreases our reliance on mitochondrial oxidative metabolism, more commonly known as the Krebs cycle. Such adaptive programs are not necessarily triggered by mitochondrial disease given the fact the hypoxic signal is absent. Hypoxia leads to a state in which oxygen delivery and consumption are simultaneously reduced, whereas in mitochondrial disease, oxygen delivery continues in the face of impaired utilization. Hence, hypoxia may represent nature's solution for overcoming mitochondrial disease pathology, both by triggering innate adaptive programs and by simultaneously limiting the oxygen over utilization. The next diagram is a good synopsis of hypoxia vs normal oxygen conditions and their manifestations. Again, one can see the many benefits of hypoxia including neurological conditions, increased life span, and better energy utilization which translates to improved performance.
The Cardiovascular and Respiratory systems also benefit from Intermittent Hypoxic Training. As was stated earlier, the bottom line for these two systems is that the Oxygen transport capacity is increased. The normal physiological response to reduced tissue perfusion is that the resulting tissue hypoxia induces HIF-1 activity, which activates transcription of genes encoding angiogenesis. These factors stimulate the remodeling of collateral blood vessels, leading to increased blood flow. HIF-1 controls oxygen delivery, by regulating angiogenesis and vascular remodeling. HIF-1 also regulates oxygen utilization by regulating glucose metabolism and redox homeostasis (the neutralization of free radicals). HIF-1 functions as a master regulator in angiogenesis and vascular remodeling process because it coordinately regulates the expression of a large number of genes whose protein products play critical roles in mediating vascular responses to hypoxia and ischemia.
WHAT ARE THE DIFFERENT TYPES OF HYPOXIA THERAPY?
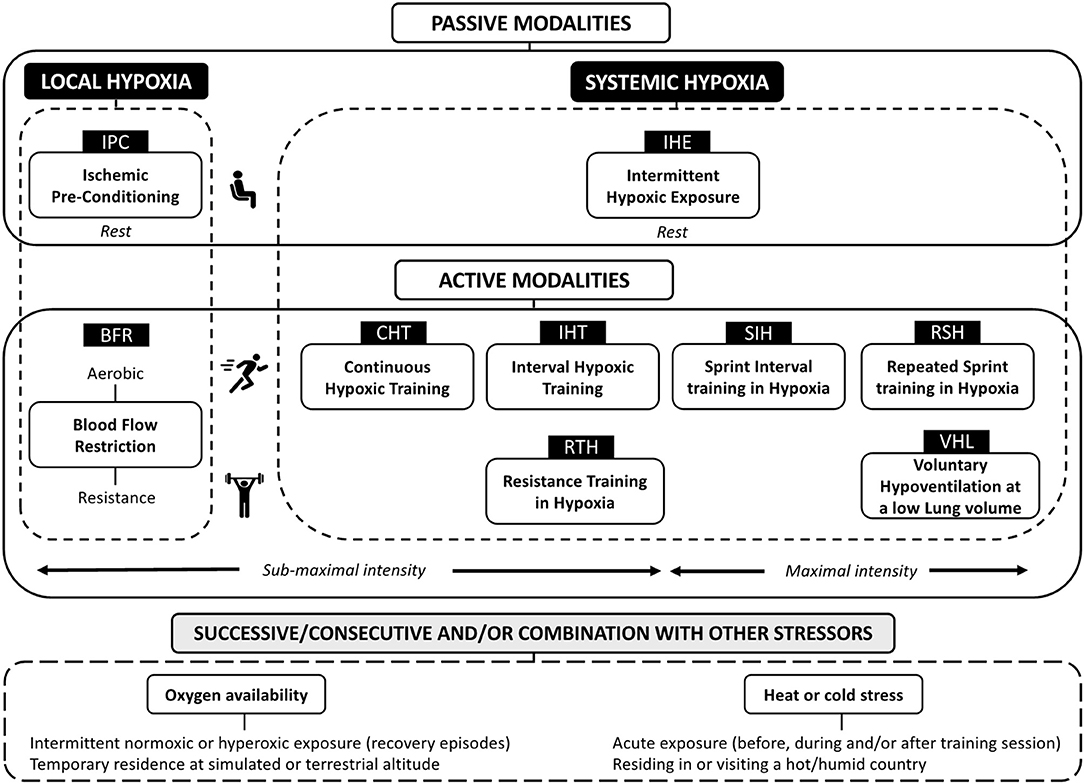
The following diagram shows the different type of hypoxia therapies. As can be seen there are two major types, local and systemic hypoxia. In the local type there is a fairly new modality called Blood Flow Restriction (BFR). BFR is exercise with the use of tourniquets which partially occlude the blood flow. Our clinic is a firm believer in this technology. However, in this particular case we are more interested in the systemic modalities which can affect the entire body. Of the systemic modalities we are most interested in the Interval Hypoxic Training. The other modalities are important and will be used from time to time. Also notice that other modalities are sometimes utilized at the end of the hypoxic session. These could include a variety of modalities including whole body cryotherapy, hyperoxia etc. more about these modalities later.
IS THE HYPOXIA DOSE AND REGIMEN IMPORTANT?
Like many aspects in science the dose of a compound or regimen can be extremely important. The following diagram shows just this phenomenon. As we can see, the effects attributed to hypoxia are dose related. This is well shown in the following diagram.
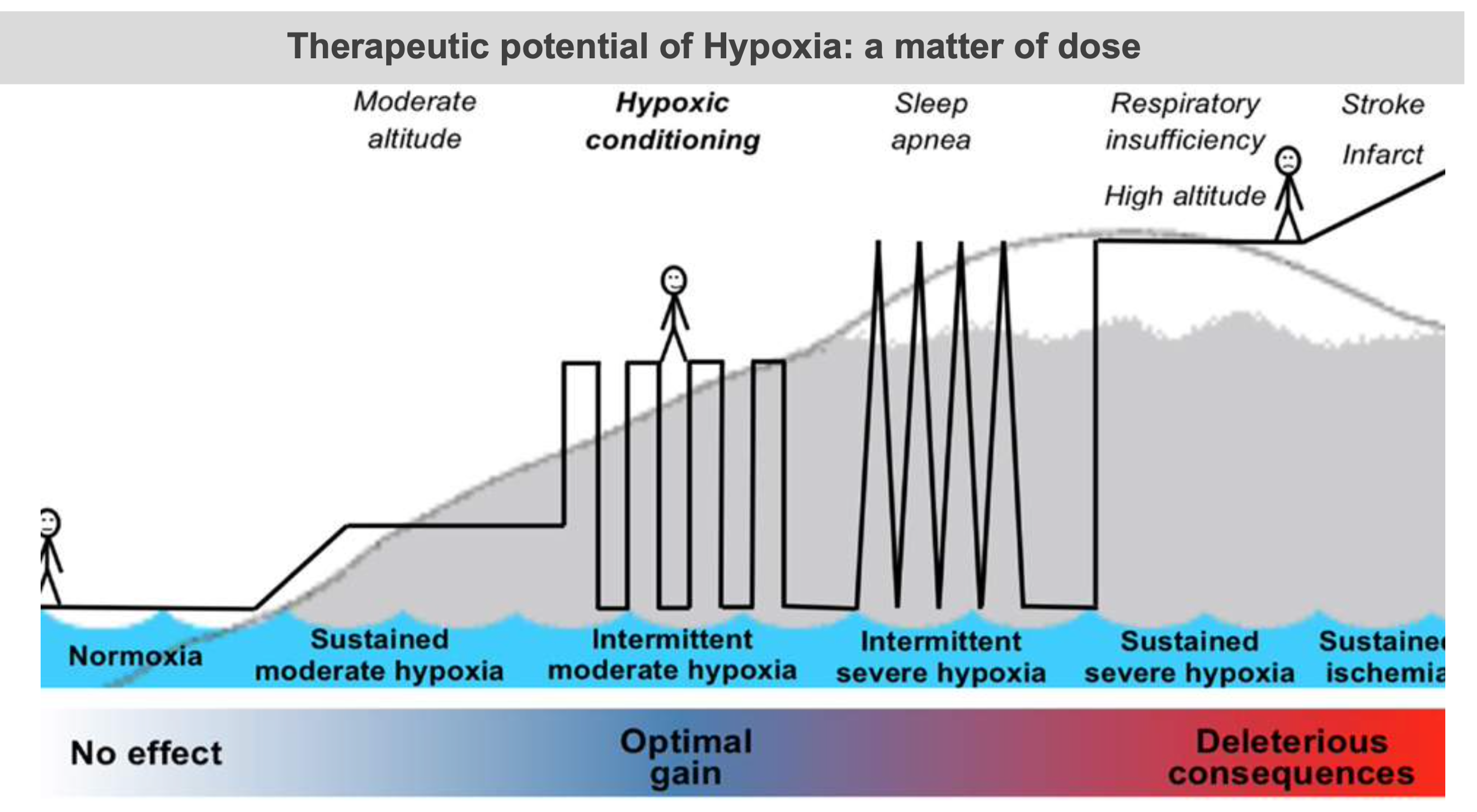
When we are at sea level there is essentially no hypoxia. We are able to see that as we move along the chart the optimal gain in health occurs with intermittent moderate hypoxia. This would occur from moderate hypoxic conditioning. Moving further along we encounter sleep apnea and finally sustained hypoxia which results in deleterious consequences. What we want to do is be in the range of intermittent moderate hypoxia. The next illustration shows the actual benefits of the proper dose of hypoxia therapy. There are many far ranging health benefits from the proper interval and concentration of Oxygen in hypoxic training. There is a wide discrepancy between the in the number of intervals and in the concentration of oxygen. A concentration of oxygen between 9% and 16% seems to be a magical number for oxygen concentration. At the same time, 15 or less episodes of hypoxia in a day seem to be the magic number for episodes. Another name for this principle is called the Hormesis effect. Hormesis refers to the beneficial effects of a treatment that at a higher intensity is harmful.
But the next question becomes what can we do to enhance the process further?
THE PRACTICAL ASPECTS OF INTERMITTENT HYPOXIC TRAINING
The difference between breathing 21 percent oxygen and 9 percent oxygen for one minute is so subtle that most people are unable to reliably report whether they were breathing normal air or low-oxygen air. Machines that provides the oxygen-reduced air are similar to those used by mountain climbers and endurance athletes who are training to compete in high-altitude environments. Intermittent hypoxia works because it prompts the body to adapt to repeated changes in oxygen levels. The reality is that there are more then 30 genes that are regulated by exposure to hypoxia stimulus. An athlete's Hematocrit level will increase [with high altitude training] but it is not the only, nor the most important, part of the phenomenon of hypoxia acclimatization.
Intermittent hypoxia works through the body’s attempt to compensate for repeated changes in oxygen levels. When the level of oxygen reaching the tissues drops, the body has “watchdogs” that respond. These so-called watchdogs are sensory neurons in your neck called the carotid body chemoreceptors, and when oxygen goes low, even for a very brief period, they are activated and tell your brain that something important is changing. This change increases the activity of a kind of neuron in the brain that contains the neurochemical serotonin. When the neurons release serotonin, it triggers neuroplasticity in motor nerve cells that supply muscles, making them work better.
The sports arena is one obvious field of performance enhancement in a legal way. The following illustration demonstrates some aspects of this concept.
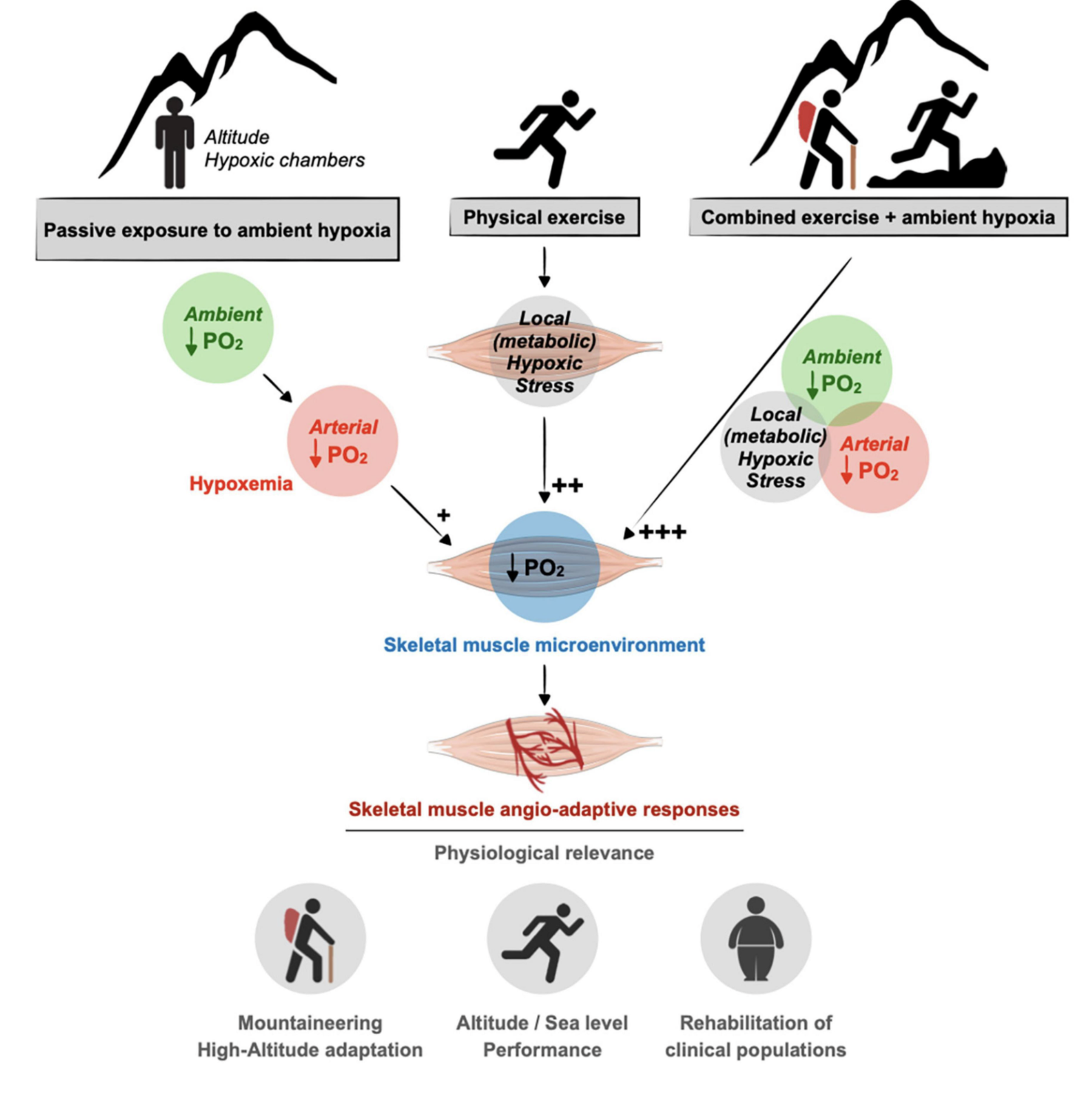
Training under hypoxic conditions, particularly IHT during a training session, improves hematological and muscle adaptations and this has been used to improve the exercise performance of athletes by sports medicine community. IHT is a modified version of the Live High Train Low (LHTL) philosophy, where an individual spends most of their time residing at high altitude prior to descending during training session. Modest hypoxia (9–16% inspired O2) and low cycle numbers (3–15 episodes per day) most often lead to beneficial effects without pathology, whereas severe hypoxia (2–8% inspired O2) and more episodes per day (48–2,400 episodes/ day) elicit progressively greater pathology. Remember as altitude increases, atmospheric pressure decreases, and although the fractional concentration of oxygen remains the same (20.9%), the partial pressure of oxygen decreases, reducing the amount of oxygen available for delivery to exercising tissues. The following chart demonstrates this. In hypoxia training we will typically target high and moderate altitude as noted on the chart.
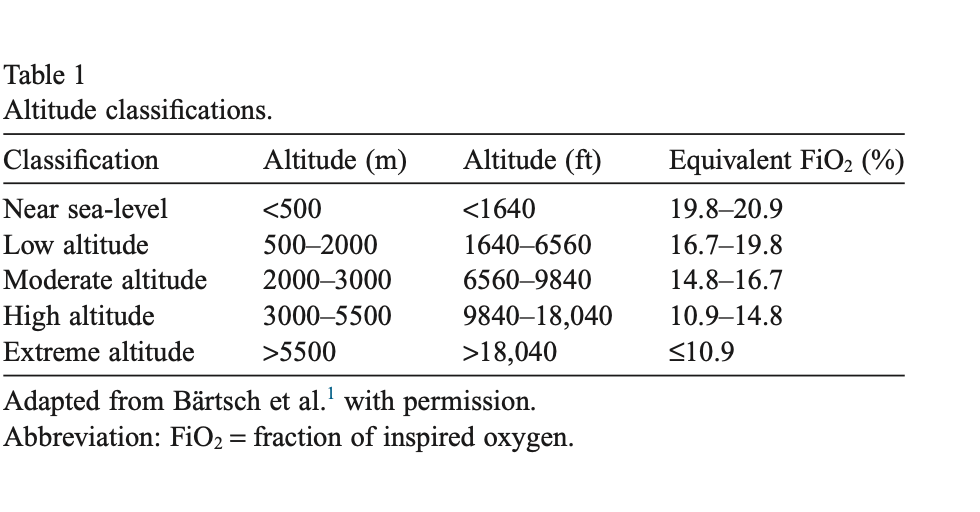
Altitude training, both in natural at altitude and artificial conditions, has been established as an effective means to improve oxygen transport, RBC volume, and VO2max (the maximum amount of oxygen that an individual can utilize during intense or maximal exercise) given sufficiently high “doses” of elevation and exposure duration. A number of different models for altitude training have been investigated, with Living High and Training Low being found to consistently improve hematological parameters and provide meaningful performance improvements in both elite and sub-elite athletes. Other altitude training models may be effective for certain groups of athletes as well, and are worth considering if an LHTL training camp is not an available option for a given athlete. However, this is all a moot point with the improvement of the new hypoxia machine devices. These devices take hypoxia training and safely to the next level. They will eventually revolutionize sports training.
Current literature has shown that repeated bouts of hypoxic training could potentially boost both biochemical and structural alterations in skeletal muscle which improves the oxidative processes in muscle cells. When IHT is completed as part of a training block, an enhancement in oxygen utilization and an improved behavior of fast twitch muscle fibers is seen. This is believed to be due to three potential mechanisms: 1. Increased vasodilation in order to improve muscle blood flow to match that of sea level exercise. 2. Improved microvascular oxygen delivery to fast twitch muscle fibers due to their high levels of fractional oxygen extraction. 3. Specific molecular adaptations (such as Hypoxic inducible factor-1) for oxygen sensing pathways. Remember, Hypoxic therapy improves many other aspects of fitness in addition to the muscles.
WHAT ARE SOME CONDITIONS THAT MAY BE IMPROVED BY HYPOXIC CONDITIONING?
There has been a great deal of clinical research on medical conditions which can be improved by hypoxic conditioning. Much of this research has taken place in Russia and Europe especially in the former “eastern bloc”. This literature has shown efficacy in Sports Performance, Cardiovascular Rehab, metabolic disorders such as diabetes, cognitive decline, and reducing fatigue and weakness while improving performance. One other interesting aspect of hypoxia training is that it seems beneficial as a technology for weight loss which has also been discussed. The studies have shown that the weight loss benefits are multifaceted and include aspects that have already been mentioned such as decreased Leptin levels which can then suppress appetite.
HOW DO WE TAKE INTERMITTENT HYPOXIA TRAINING TO THE NEXT LEVEL?
Our clinic will take things one step further by utilizing both hypoxia and hyperoxia during the same session. We will be utilizing a specially designed machine that incorporates both hypoxia and hyperoxia. This device provides personalized Intermittent Hypoxia-Hyperoxia Training (IHHT). This training involves repeated short-term hypoxia (10-15% O2), interrupted by brief periods of recovery by means of short-term hyperoxia (30-35% O2). This is a departure from the typical intermittent training which typically only involves hypoxia and sometimes normal oxygen content (21%).
Intermittent Hypoxic Training will benefit elite athletes, both professional and non-professional. The question is how can we improve upon the process. The following diagram sheds some light on how this can be accomplished by utilizing hypoxia and hyperoxia (high oxygen content) in the same treatment plan. We can see that hypoxia and hyperoxia both have benefits. When we combine both of these modalities the benefits are greatly increased. This becomes a disruptive technology by its ability to provide personalized treatment for each patient by utilizing a method of Interval Hypoxia-Hyperoxia Treatment under biofeedback control.
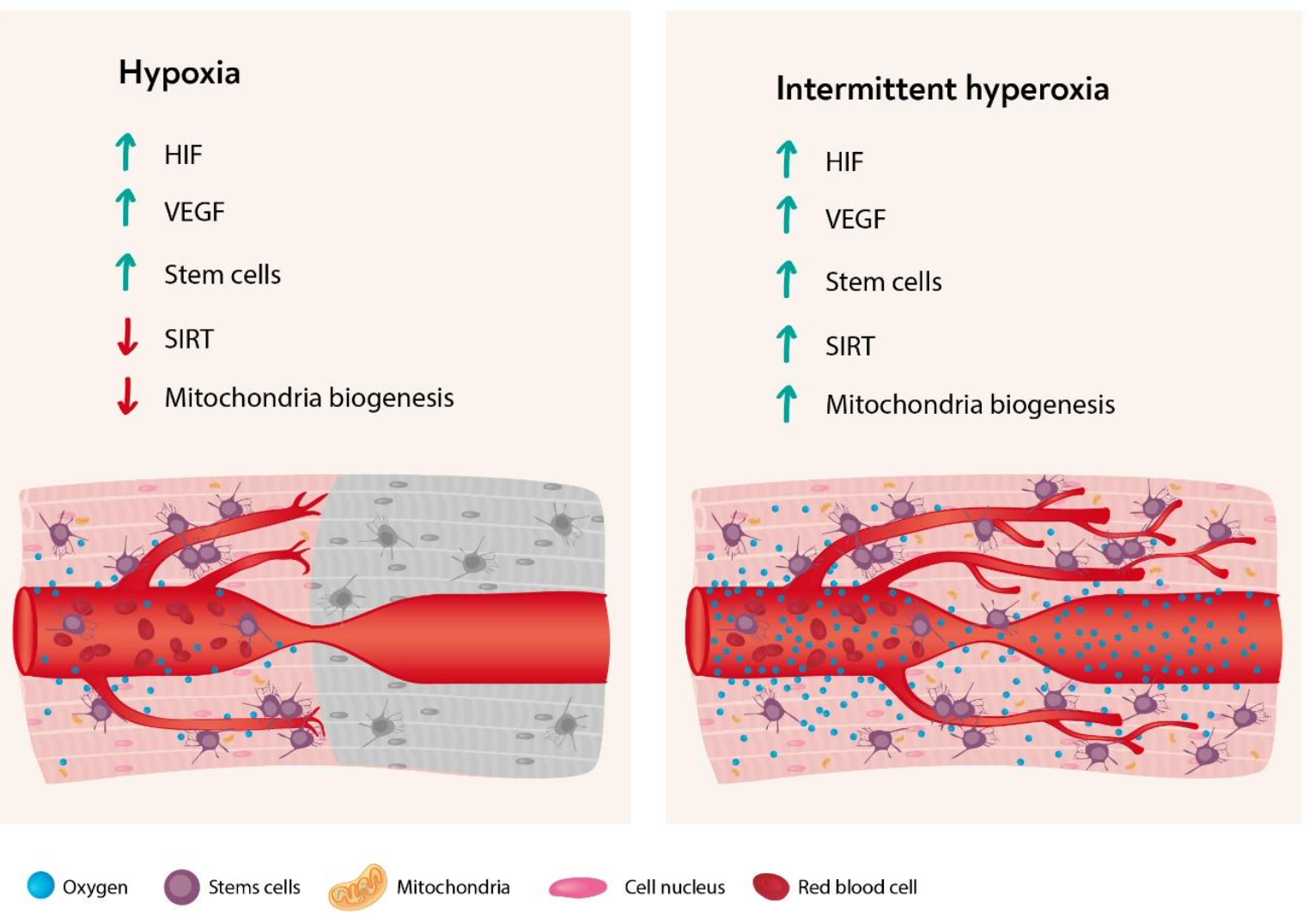
The main idea of the Interval Hypoxic Treatment (IHT) method is repeated reduction of blood oxygen to the individual intermingled with recovery intervals. A reduction in oxygen level stimulates activity of protective proteins such as antioxidant enzymes, heat shock proteins, Iron-regulating proteins, repair enzymes, and growth factors. This begins by starting a cascade of reactions that leads to hypoxia adaptation and new defensive mechanisms which produce positive physiological changes. When this training is combined with hyperoxia many different pathways are stimulated. Intermittent hypoxic–hyperoxic training (IHHT), has been proposed as being associated with even more beneficial effects than IHT. The Normoxia periods are replaced by moderate hyperoxic periods with 30%–40% oxygen resulting in a faster recovery of oxygen desaturation (Oxygen desaturation means that the percentage of oxygen in your blood is lower than it should be). Taking a cue from a recent Israeli study which involved Hyperbaric Oxygen, the intermittent hypoxia-hyperoxia episodes can actually increase telomere length in the cells of our immune system. This is a big deal since it is making the cells of our immune system younger. A younger and healthier immune system makes for a healthier patient. It is helping to diminish immuno-senescence, which involves the aging of our immune system.
Oxygen availability has a crucial impact on the diffusion of O2 into muscle cells and on the time required for recovery of phosphocreatine. Phosphocreatine is a naturally occurring substance that is found predominantly in our skeletal muscles. Its primary purpose within the body is to serve in the maintenance and recycling of adenosine triphosphate (ATP) for muscular activity like contractions. With more and more pronounced hypoxia, the changes in our arterial oxygen saturation stimulate cardio-respiratory efforts designed to compensate for the reduction in systemic O2 transport and counteract impairment of performance and muscle activity. At the same time, breathing hyperoxic air elevates the amount of oxygen dissolved in the arterial plasma, thereby potentially accelerating recovery. In recent years, the physiological responses of athletes to high intensity exercise with intermittent hypoxic training as well as repeated sprints in hypoxia, have attracted increasing scientific interest. There are a number of other benefits from hypoxia-hyperoxia. One major that it seems to shorten the recovery period after sports injury and aiding the rehabilitation of athletes with overtraining syndrome.
HYPOXIA AND STEM CELLS
Last but not least is the effect hypoxia has on stem cells. The following illustration shows some of the relationships between hypoxia and stem cells. The illustration shows a cell with its mitochondria and nucleus. Oxygen is an important component of the cellular micro-environment, serving as both metabolic substrate and signaling molecule. Oxygen has been shown to have a variety of effects on embryonic and adult stem cells. Hypoxia has a role in regulating stem cell biology specifically focusing on growth, maintenance of pluripotency (the ability to produce many different types of cells), differentiation, and production of growth factors. Actually, in our regenerative procedures in the office, we subject the regenerative cells to hypoxia typically in a vacuum in a test tube. This is called in vitro or outside the body. While intermittent hypoxia training subjects the regenerative cells in the body to hypoxia which is called in vivo (in the body). The illustration is a good example of some of the benefits that hypoxia brings to the table as far as stem cells are concerned.
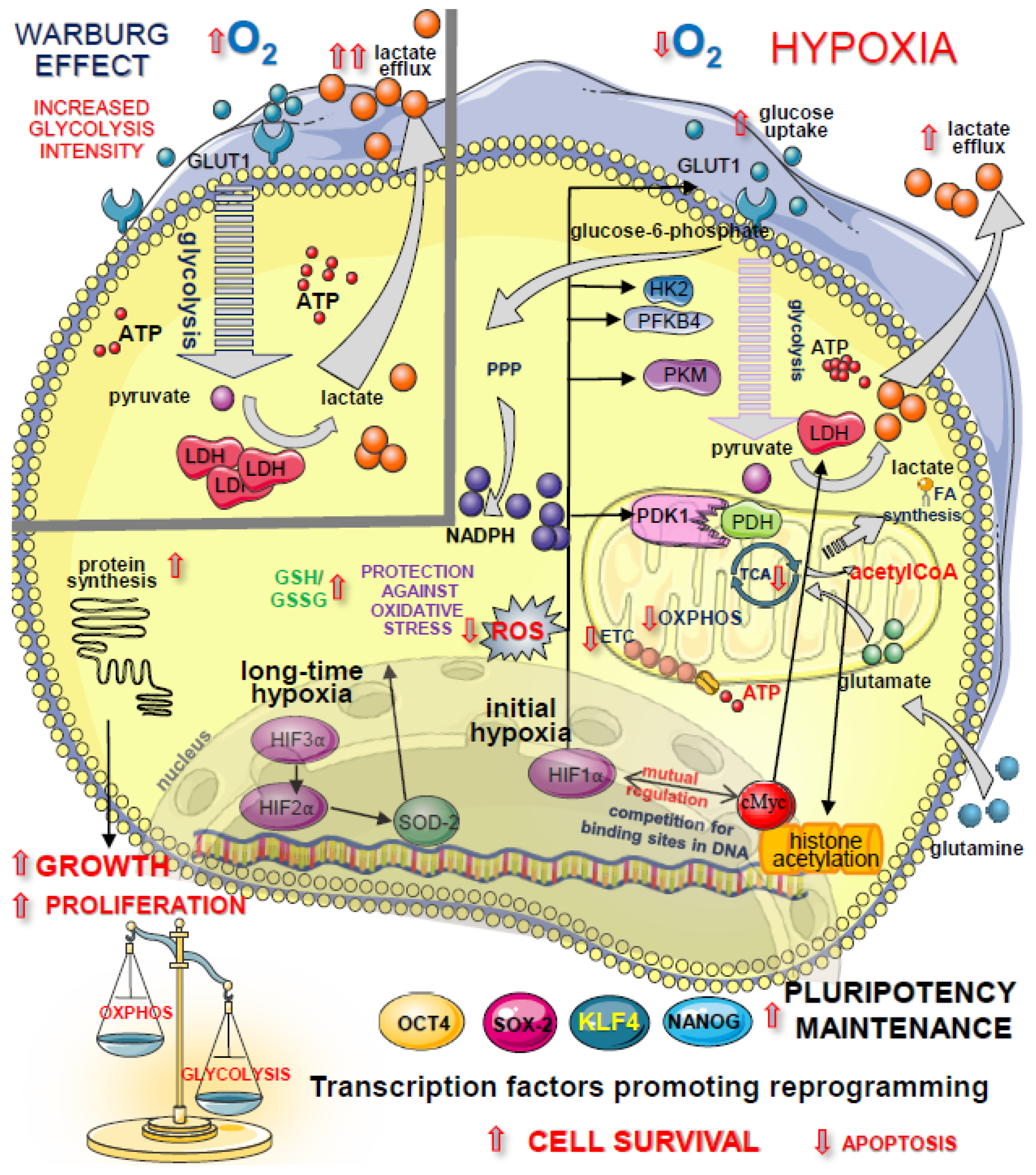
It actually is a review of many of the aspects that have previously been mentioned in this article. Additionally, we think that hypoxia treatments would have a beneficial effect on V cells found in the body. These are specialized cells that we each have. They are called Very Small Embryonic Like Stem Cells. These cells are pluripotent meaning they can form many different types of cells. Hypoxia stimulates these cells to maintain their pluripotency.
SOME INTERESTING FACTS ABOUT HYPOXIA TRAINING
The Hypoxia Therapy method is very natural, as it utilizes unique genetically installed human body phenomena. We can rapidly compensate for disruptions at all levels caused by decreases in oxygen intake and adapting to its newest environment. So-called ‘super-recovery’ follows total recovery of a disrupted function so that body’s resistance to a specific factor improves. As we are developing in our mother womb, body development takes place in a low PO2 environment similar to an altitude of 16,000-19000 ft. above sea level. Furthermore, PO2 values in the womb and fetal tissues change cyclically. Ability of the fetus to super-recover in response to decreased PO2 is an aspect of specific fetus training and forms its ability to resist external factors following birth. So, in a way we are turning back the clock with Intermittent Hypoxic Training. IHT is a convenient way to tune the oxygen transport system and increase the power of the oxidative process. It relates to the fact that the oxygen transport system, including breathing, cardiovascular systems, blood, multilayered regulators and cell breath systems dominate in terms of responsibility for adaptive changes. These effects are realized also during continuous intensive physical exercises of aerobic nature of longer than 30 minutes. Hypoxic training is easy to perform, which along with the absence of limitations is another benefit for patients, especially those overweight or with metabolic syndrome.
Highland communities typically enjoy a 15–20 years longer lifespan. Median lifetime of Hunz valley inhabitants, in the Karakorum mountains (Pakistan), at an elevation 8,000 ft. is 120 years. Non-athletes, including the elderly, have also been shown to benefit with improvements in various markers of aerobic fitness, circulation and breathing
Observations from populations of the Andes indicate that both coronary heart disease and myocardial infarction are uncommon among residents at high altitude. In a consecutive series of necropsies performed at an elevation of 14,000 ft., there was no case of myocardial infarction or of even moderate coronary artery disease.
In Switzerland, the age-standardized mortality rates (per 100,000 person-years) from Ischemic Heart Disease decreased in men from 289 below 1,000 ft. of altitude to 242 at altitudes above 5,000 ft. and in women from 104 at altitudes below 1,000 ft. to 74 at altitudes between 5,000 ft. to 6500 ft.
WHAT HAPPENS WHEN INTERMITTENT HYPOXIA TRAINING IS COMBINED WITH OTHER MODALITIES?
We will combine IHT with other modalities that should enhance it further. This would include Hyperoxia treatments. Some other modalities would include Hyperbaric Oxygen, Whole Body Cryotherapy, Red Light Sauna, and a few other modalities. How we incorporate them is propriety. Also, certain dietary supplements such as Ginkgo biloba, coenzyme Q10, and beetroot juice can increase oxygenation through enhanced blood flow while branched-chain amino acids and omega-3 fatty acids can improve maximum oxygen consumption Vo2max. These will represent a portion of our protocol.
SOME FINAL THOUGHTS ON INTERMITTENT HYPOXIA TRAINING
Intermittent Hypoxia Training will be a disrupting technology. Like most things it has to be performed properly and safely. We would not settle for anything less. We will use the latest state of the art machine for hypoxia training. At the same time, it will also utilize hyperoxia. It will consistently monitor the patient and make individual adjustments to best suit the patient and his therapy.